Last week I was able to attend a lecture marking the retirement of Professor Alan Fenwick, Director of the Schistosomiasis Institute. It was a fascinating insight into both a remarkable endeavour and a remarkable man, which I want to share with the Giving What We Can community. A huge thank you to Alan for the lecture and for providing the images in this post for me to use.

Professor Fenwick treated us to a retrospective of a career spanning five decades, which took him from a Chemistry degree to spearheading the campaign to eradicate a terrible disease. You can watch the full lecture on YoutTube.
When he joined the Liverpool School of Tropical Medicine to do a PhD, it was with the aim of developing a molluscicide to kill the snails that are the intermediate hosts for the schistosome. This work took him to the field in Arusha, developing pesticides with the Tropical Pesticide Research Institute, and to Sudan with the Wellcome Trust, collaborating with teams working on malaria control. It was here (between mountwaain climbing, golf, writing pantos, playing cricket and Scottish dancing) in 1977 that they conducted trials of a new agent – Praziquantel. It was only 40 years ago that we first we had an effective treatment for schistosomiasis!
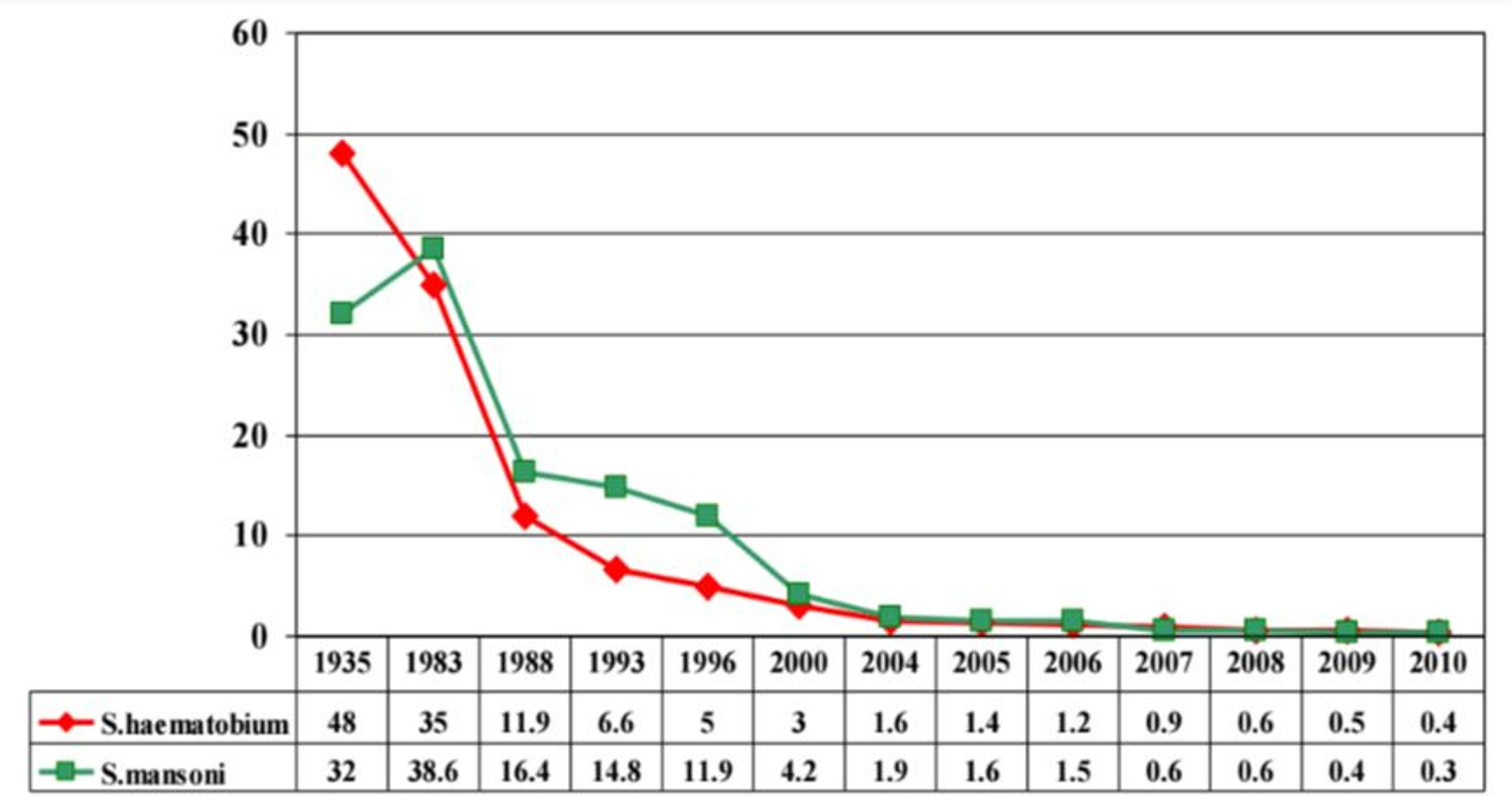
After leaving Sudan, Prof Fenwick became chief of party for a group charged with eliminating schistosomiasis as a health problem in Egypt. It is astonishing to see the prevalence of this disease plotted over time – from over 35% in 1983, and down by an order of magnitude to less than 2% at the end of his time there (and less than 0.5% in 2010). I think sometimes we lose sight of what a tremendous achievement it is to take a disease affecting literally 1 in 3 people and make it rare in the course of a lifetime.
At the end of his time in Egypt, Prof Fenwick acknowledges he probably could have retired. Instead, he turned his expertise, eminence and a lifetime of connections to do more good. He sought a grant from the Gates Foundation to work on schistosomiasis elsewhere. A modest request for $50 million was unfortunately turned down, but when a meagre $34 million was offered, Prof Fenwick “reluctantly agreed” and founded the Schistosomiasis Control Initiative.
Here we heard just what a unique and remarkable position he was in to do this work. He made contact with Dr Narcis Kabatereine, who many years ago had introduced himself at a meeting as “the Ugandan schistosomiasis control officer, with no budget”. I can’t do justice to the story of their search for the Minister of Health, whose agreement was critical to release the funding for treatment, but in telling the story, Prof Fenwick gave some demonstration of why he has been such a successful organizer and fundraiser, as well as evidence of the value of playing golf. Together with Dr Kabatereine, SCI developed a national program to eradicate schistosomiasis in Uganda, and Dr Kabatereine remains an adviser to SCI on African capacity building.
Prof Fenwick acknowledged the immense contribution of the pharmaceutical industry to global health and the control of neglected tropical diseases. Merck KGaA committed 20 million tablets of praziquantel per year in 2007: that donation has now reached 250 million tablets a year. GSK and Johnson & Johnson are likewise donating hundreds of millions of tablets a year. This is both an incredible gift, and a challenge. The safe and effective distribution of these treatments is an enormous undertaking.
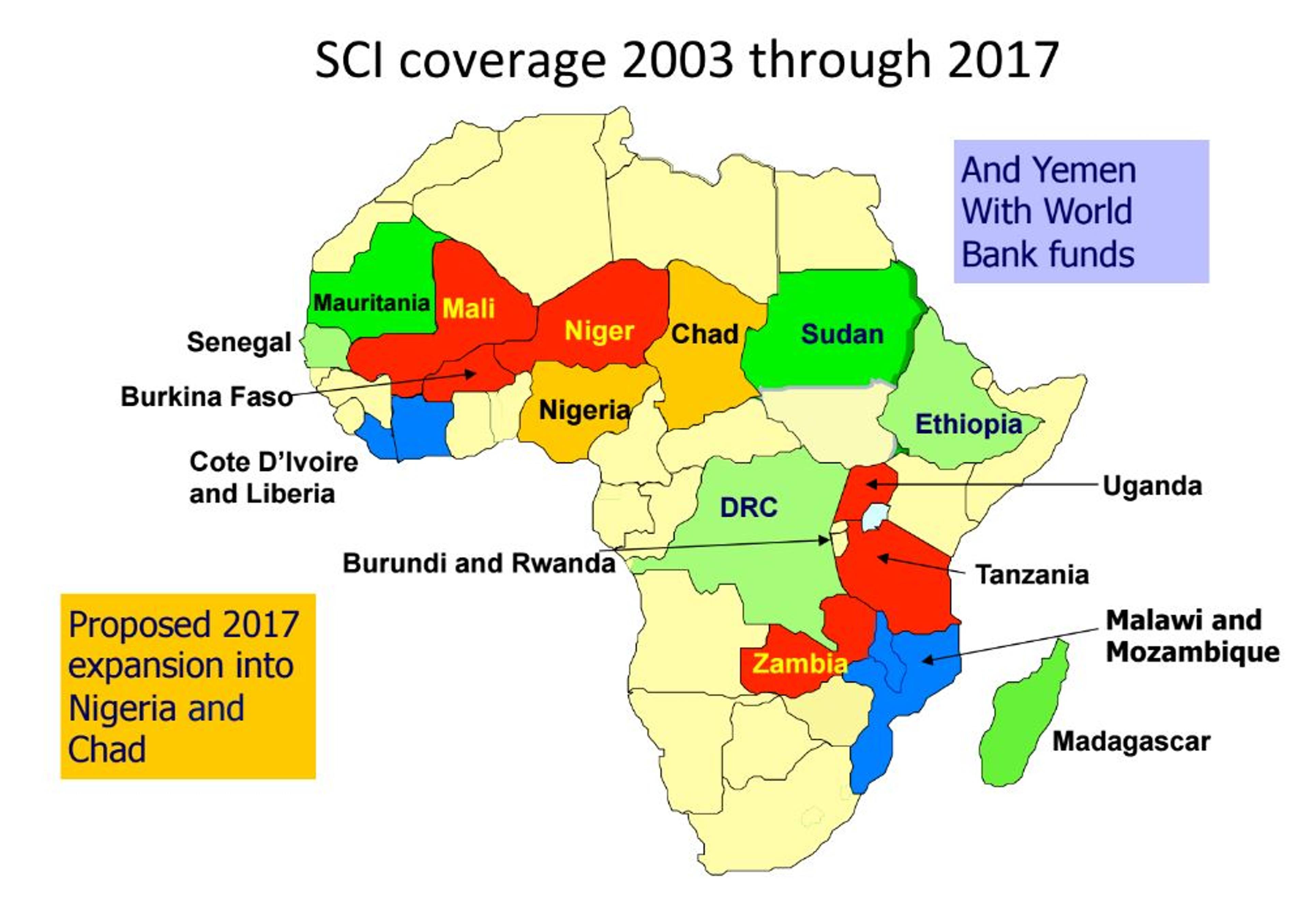
About half of SCI’s work in distributing these treatments is funded by large government grants. Individual donors fund the remainder. It is here that our histories meet: Prof Fenwick describes a meeting with “some Oxford philosophers who were interested in cost effective giving”, and it wasn’t much later he was attending the launch of Giving What We Can in 2009. Since then, SCI has benefited from a ‘new wave of donors’, who cite GWWC, Givewell and The Life You Can Save as their sources. Good Ventures, the ENDFUND and some very generous individual donors have also made a huge difference to the operational capacity of SCI, as we can see in a map showing the earliest mass deworming operations (in blue), their next expansion (in red) and current coverage (red, blue and green). Bear in mind that in 2002, in Africa only Egypt had a schistosomiasis control programme.
Prof Fenwick is modest about his contributions, as evidenced by mention of his OBE – which he deprecatingly describes as recognition of “Other Buggers’ Efforts. But it’s clear he has led a charge to drastically change the impact of an actual scourge. It was clear from the pictures he posted throughout that the face of this work has changed over 50 years. The team taking over the reins, who will be the new champions of Neglected Tropical Diseases. Afterwards, I had a chance to talk to Dr Sarah Nogaro, a SCI programme manager working with both established distribution programme in Burundi, and new programmes in Madagascar. I left with a real sense of optimism: these are experts guiding local action, supporting locally led deworming. They have passion, and a huge commitment to the work they are doing.
A moment that stuck with me was Prof Fenwick’s remark, in acknowledging his mentors, that “everybody has somebody in their life without whom they would never get where they are going”. Mostly, we get to have that kind of impact on just a few people. But disease can stop people from getting anywhere. There are millions of people who, without the work of SCI and the funding of its supporters, would probably not have been treated for worms, and whose progress has been forever changed. What an utterly outstanding project to be a part of, and what an extraordinary man it is, who has given so much to that project.
We wish him every joy in a well-earned retirement.
